Epidemiological Similarities and Differences Between Toxoplasmosis and Schizophrenia
Epidemiologically, there are at least eight areas of similarity between toxoplasmosis and schizophrenia. There are also at least three areas in which epidemiological aspects are dissimilar.
The areas of similarity are as follows:
Familial and genetic aspects
The fact that schizophrenia is familial, as demonstrated by family, twin, and adoption studies, is one of the most salient features of this disease. The explanation for this familial pattern is widely assumed to be genetic, and hundreds of candidate predisposing genes have been identified. Many of the candidate genes predisposing to schizophrenia have been shown to be activated by Toxoplasma infection in cell cultures and in experimental animals. (For a detailed analysis of the effect of T. gondii on genes which have been linked to schizophrenia see Carter CJ. Toxoplasmosis and polygenic disease susceptibility genes: Extensive Toxoplasma gondii host/pathogen interactome enrichment in nine psychiatric or neurological disorders. J Pathogens. 2013;2013:965046). Of particular importance was the activation of microRNAs such as mi132 and mi137 since these microRNAs have been implicated in schizophrenia by genetic studies. Additional studies have confirmed the existence of genetic variants in humans that partly determine the outcome of exposure to T. gondii.52-54
Toxoplasmosis has also been observed to be familial but not necessarily for genetic reasons. A clustering of T. gondii infections has been noted in families of congenitally infected infants.1 A familial pattern to the disease has also been observed, both from having common food exposure and from common exposure to an infected cat.2-3 In one study of family transmission, it was found that in half of the families in which one person becomes infected with acute toxoplasmosis, as second member of the family also becomes infected.4 Animal models of toxoplasmosis have demonstrated that genes influence the susceptibility of animals to T. gondii infection.5-6 It is also known that mice with chronic T. gondii infections can pass the infection to their offspring for as many as five successive generations in a pseudogenetic pattern.7-8 See section on vertical transmission, above.
Age of onset
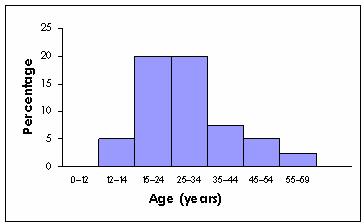
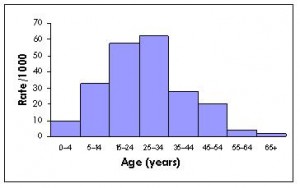
Studies have shown that the peak onset of schizophrenia occurs between the ages of 20 and 30, with results varying depending on whether “onset” is defined by the first symptoms, treatment or hospitalization. Studies have shown a similar peak onset for individuals with recently acquired, adult-onset toxoplasmosis, clinically suggested by lymphadenopathy (see Fig. 1).9-10 The peak age of primary infections with T. gondii was also shown in a Dutch study to be “adolescence and early adult life,” with a peak at ages 17 to 20.11
Figure 1. Comparison of age of onset of schizophrenia and toxoplasmosis
Age of onset of schizophrenia as determined by first admission
Age of onset of adult toxoplasmosis as determined by lymphadenopathy
Males get sick at a younger age than females
It is clearly established that males develop schizophrenia at an average younger age than females. In studies done in England, the mean age at first admission for schizophrenia was 28.0 for males and 31.8 for females.12 The pattern is similar for adult-onset toxoplasmosis; in one study, the mean age of onset was 27.7 for males and 31.9 for females.13 In another study, three times more males than females became infected under age 15.14
Socioeconomic status and household crowding
In the United States, studies have demonstrated that the prevalence of schizophrenia is higher in individuals who are poorer and who live in more crowded households.15-16 Similarly, the prevalence of antibodies to T. gondii has been shown to be higher in individuals who are poorer and who live in more crowded households.17
Seasonal variation
Individuals who develop schizophrenia are more likely to be born in the winter and early spring months. This pattern has been confirmed in over 100 studies in both the northern and southern hemispheres. The schizophrenia birth excess is 5-8 percent and is more marked in colder than warmer states in the U.S.18 and in colder than warmer countries in Europe.19 In addition to having a winter and early spring excess of births, individuals who later develop schizophrenia have a fall deficit of births that is as statistically significant as their winter-spring excess.
Nine studies of the seasonality of toxoplasmosis have been carried out. Two studies assessed the acquisition of antibodies to T. gondii in large numbers of pregnant women in Slovenia20 and Austria21; both studies reported a twofold increase in seroconversion in winter months compared to summer months. A study in the Netherlands looked retrospectively at the birth months of 532 patients with ocular toxoplasmosis and reported a significant increase in May (with assumed seroconversion in March, April, and May) and a significant deficit in November.22 An American study looked at the seasonality of acute toxoplasmic lymphadenopathy and reported that the peak months were December and then September.23
Four studies looked at the seasonality of receipt of lab specimens for testing for T. gondii. Almost all were cases of suspected ocular toxoplasmosis or toxoplasmic lymphadenitis. Such studies are an indication of the clinical manifestations of toxoplasmosis. A German study examined 30,000 specimens received between 1968 and 1971 and reported: “Acute toxoplasmosis has a typical annual cycle of incidence, occurring more frequently in the winter and spring months, with a clear reduction in the summer and autumn”.24 A UK study reported a peak in such lab reports from November to February (winter), with a deficit in September25, but another UK study reported no seasonal pattern.26 A similar study of lab reports in Canada reported a relatively even distribution of reports for all months except September-November, when there was a deficit.27 Finally, a study from Serbia reported that among 391 cases of recent lymphadenopathy caused by T. gondii, the acute infections occurred more often between October and March (p=0.05).28
Thus, it appears that human T. gondii infections occur more commonly in the winter months, with a deficit in the fall months. This coincides with the seasonal pattern of individuals who develop schizophrenia. Given the multitude of ways in which T. gondii can be acquired in humans, how might the two be linked? One possibility is as a consequence of cats spending more time in homes in winter months than in summer months. Infected cats would thus be excreting their oocysts into the home environment during those months, thus potentially infecting a woman in the last months of pregnancy and/or a newborn child. This might also explain why schizophrenia birth seasonality is more pronounced in colder states and colder countries, where cats are more likely to be indoors.
Another possibility is that infection with T. gondii and schizophrenia might be linked through the seasonality of cat births. Cats are born throughout the year, but in the U.S. cat births peaked in March-August in one study29 and in March-May in another study.30 Cats most commonly become initially infected with T. gondii as kittens, when they first start hunting, which is usually 6-10 weeks after being born. It is during the approximately 2 weeks when they are initially infected that they excrete oocysts and thus may infect humans. The peak months when kittens are born, March-May, could thus produce May-July as the months during which the newborn kittens would be most likely to be infective. A German study of oocyst shedding by cats found that it occurs most commonly in the summer and fall, thus being consistent with the spring birth of kittens.31 This does not correspond with the peak births of individuals with schizophrenia; thus, this explanation seems less likely. A May-July peak of infectious kittens would correspond with the first trimester of pregnancy for women giving birth in the winter months, but these women would be expected to give birth to offspring who have the congenital toxoplasmosis syndrome.
Association with stillbirths
An increase in stillbirths among mothers with schizophrenia has been reported in five studies.32-36 However, it was not found in a sixth study (37). An increase in stillbirths has also been documented among women infected with T. gondii during pregnancy.38
Geographic low-prevalence toxoplasmosis regions
As has been demonstrated on isolated islands, toxoplasmosis does not exist in places where there are no felines. In areas where felines are rare, the prevalence rates of both toxoplasmosis and schizophrenia appear to be low. The best example is probably the highlands of Papua New Guinea, where until recently, domesticated cats were virtually nonexistent and wild felines comparatively rare. In this area, the percentage of people with antibodies to T. gondii was reported to be 2 percent or less.39 A 1973 study of the prevalence of schizophrenia in this area also reported it to be among the lowest in the world.40
Historical trends
Although cats were kept as pets in ancient Egypt, their modern domestication began only in the mid-eighteenth century and then increased rapidly.41 Some people believe that schizophrenia was a rare disease prior to the mid-eighteenth century but then increased rapidly in incidence. Thus, the increase in keeping cats as pets and the increase in schizophrenia would have coincided.42
The areas in which epidemiological aspects of toxoplasmosis and schizophrenia are unclear or dissimilar are as follows:
Urban-rural differences
Almost all studies have reported that being born in, or having lived as a child in, an urban area, compared to a rural area, confers an increased risk of later being diagnosed with schizophrenia.43 By contrast, some studies of antibodies to T. gondii have reported them to be more common in individuals in urban areas, but other studies have reported them to be more common in individuals in rural areas. One summary concluded that such studies have shown “no consistent pattern, with rural predominance in some and urban in others”.44 Specifically for oocyst transmission, however, there are indications that this occurs more in urban than in rural areas, based on studies of sandbox contamination.45
Geographic high-prevalence toxoplasmosis regions
Although geographic areas with a low prevalence of T. gondii antibodies also have a low prevalence of schizophrenia, the opposite is not the case. Individuals in countries such as France, Ethiopia, and Brazil have a high prevalence of antibodies to T. gondii. In France and Ethiopia, the high infection rates are thought to be attributable to the cultural custom of eating undercooked or uncooked meat; in Brazil, the high rate has been attributed to water supplies contaminated with feline oocysts as well as to undercooked meat consumption.46-47 By contrast, studies of the prevalence of schizophrenia in these countries have not suggested that they have unusually high rates by world standards.
Historical trends
There are multiple reports that the seroprevalence of toxoplasmosis has decreased sharply in the United States and Europe in the past forty years.48 It has been speculated that this is because of the increased use of frozen meat, since freezing kills the tissue cysts, and better food hygiene in general.49-51 By contrast, there are no reports of a sharp decrease in the prevalence of schizophrenia in either the United States or Europe.
References
- Contopoulos-Ioannidis D, et al. Clustering of Toxoplasma gondii infections within families of congenitally infected infants. Clinical Infectious Diseases. 2015; DOI: 10.1093/cid/civ721.
- Stagno S, Dykes AC, Amos CS, et al. An outbreak of toxoplasmosis linked to cats. Pediatrics. 1980;65:706–712.
- Sacks JJ, Roberto RR, Brooks NF. Toxoplasmosis infection associated with raw goat’s milk. JAMA. 1982;248:1728–1732.
- Contopoulos-loannidis DG, Maldonado Y, Montoya JG. Acute Toxoplasma gondii infection among family members in the United States. Emerg Infect Dis. 2013;19:1981-1984.
- Johnson J, Suzuki Y, Mack D, et al. Genetic analysis of influences on survival following Toxoplasma gondii infection. Int J Parasitol. 2002;32:179–185.
- Blackwell JM, Roberts CW, Alexander J. Influence of genes within the MHC on mortality and brain cyst development in mice infected with Toxoplasma gondii : kinetics of immune regulation in BALB H-2 congenic mice. Parasite Immunol. 1993;15:317–324.
- Beverley JKA. Congenital transmission of toxoplasmosis through successive generations of mice [letter]. Nature. 1959;183:1348–1349.
- Owen MR and Trees AJ. Vertical transmission of Toxoplasma gondii from chronically infected house [Mus musculus] and field [Apodemus sylvaticus] mice determined by polymerase chain reaction. Parasitology. 1998;116:299–304.
- Häfner H, Riecher-Rössler A, an der Heiden W, et al. Generating and testing a causal explanation of the gender difference in age at first onset of schizophrenia. Psychol Med. 1993;23:925–940.
- Jackson MH, Hutchinson WM. The prevalence of Toxoplasma infection in the environment. Adv Parasitol. 1989;28:55–105.
- Van der Veen J, Polak MF. Prevalence of Toxoplasma antibodies according to age with comments on the risk of prenatal infection. J Hyg (Camb). 1980;85:165–174).
- Watt DC, Szulecka TK. The effect of sex, marriage and age at first admission on the hospitalization of schizophrenics during 2 years following discharge. Psychol Med. 1979;9:529–539.
- Ryan M, Hall SM, Barrett NJ, et al. Toxoplasmosis in England and Wales 1981 to 1992. Commun Dis Rep CDR Rev. 1995;5:R13–21.
- Beverley JKA, Fleck DG, Kwantes W. Age-sex distribution of various diseases with particular reference to toxoplasmic lymphadenopathy. J Hyg (Camb). 1976;76:215–228.
- Regier DA, Farmer ME, Rae DS, et al. One-month prevalence of mental disorders in the United States and sociodemographic characteristics: the Epidemiologic Catchment Area study. Acta Psychiatr Scand. 1993;88:35–47.
- Schweitzer L and Su E-H. Population density and the rate of mental illness. Am J Public Health. 1977;67:1165–1172.
- Kruszon-Moran D, McQuillan GM. Seroprevalence of six infectious diseases among adults in the United States by race/ethnicity: data from the third National Health and Nutrition Examination Survey. Adv Data. 2005;352:1–9.
- Torrey EF, Torrey BB, Peterson MR. Seasonality of schizophrenic births in the United States. Arch Gen Psychiatry. 1977;34:1065-1070.
- Torrey EF, Miller J, Rawlings R, et al. Seasonality of births in schizophrenia and bipolar disorder: a review of the literature. Schizophr Res. 1997;28:1–38.
- Logar J, Soba B, Premru-Srsen T, Novak-Antolic Z. Seasonal variations in acute toxoplasmosis in Slovenia. Clin Microbiol Infect. 2005;11:852-855.
- Sagel U, Mikolajczyk RT, Kramer A. Seasonal trends in acute toxoplasmosis in pregnancy in the federal state of Upper Austria. Clin Microbiol Infect. 2010;16:515-517.
- Meenken C, Rothova A, Kijlstra A, et al. Seasonal variation in congenital toxoplasmosis [letter]. Br J Ophthalmol. 1991;75;639.
- Contopoulos-Ioannidis D, et al. Seasonal variation of acute toxoplasmic lymphadenopathy in the United States. Epidemiol Infect.2014; Nov 20:1-5.
- Braveny I., et al. Untersuchungen zur Epidemiolgie der Toxoplasmose. Dtsch Med Wschr. 1973; 98: 535-539.
- Bannister B. Toxoplasmosis 1976-80: review of laboratory reports to the Communicable Disease Surveillance Centre. J Infect. 1982;5:301-306.
- Ryan M, Hall SM, Barrett NJ, et al. Toxoplasmosis in England and Wales 1981 to 1992. CDR Review: Communicable Disease Report. 1995;5:R13-22.
- Tizard IR, Fish NA, Quinn JP. Some observations on the epidemiology of toxoplasmosis in Canada. J Hyg (Camb). 1976;77:11-21.
- Bobic B, Klun I, Nikolic A, et al. Seasonal variations in human Toxoplasma infection in Serbia. Vector-Borne Zoonotic Dis. 2010;10:465–469.
- Reif JS. Seasonality, natality and herd immunity in feline panleukopenia. Am J Epidemiol. 1976;103:81-87.
- Nutter FB, Levine JF, Stoskopf MK. Reproductive capacity of free-roaming domestic cats and kitten survival rate. J Am Vet Med Assoc. 2004;225:1399-1402.
- Schares G. et al. Seasonality in the proportions of domestic cats shedding Toxoplasma gondii or Hammondia hammondi oocysts is associated with climatic factors. International Journal of Parasitology. 2016; http://dc/doi.org/10.1016/j.ijpara.2015.12.006.
- Sobel DE. Infant mortality and malformations in children of schizophrenic women. Psychiatr Q. 1961;35:60–65.
- Rieder RO, Rosenthal D, Wender P, et al. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry. 1975;32:200–211.
- Modrzewska K. The offspring of schizophrenic parents in a North Swedish isolate. Clin Genet. 1980;17:191–201.
- Nilsson E, Lichtenstein P, Cnattingius S, et al. Women with schizophrenia: pregnancy outcome and infant death among their offspring. Schizophr Res. 2002;58:221–229.
- Bennedsen BE, Mortensen PB, Olesen AV, et al. Congenital malformations, stillbirths, and infant deaths among children of women with schizophrenia. Arch Gen Psychiatry. 2001;58:674–679.
- Jablensky AV, Morgan V, Zubrick SR, et al. Pregnancy, delivery, and neonatal complications in a population cohort of women with schizophrenia and major affective disorders. Am J Psychiatry. 2005;162:79–91.
- Sever JL, Ellenberg JH, Ley AC, et al. Toxoplasmosis: maternal and pediatric findings in 23,000 pregnancies. Pediatrics. 1988;82:181–192.
- Wallace GD, Zigas V, Gajdusek DC. Toxoplasmosis and cats in New Guinea. Am J Trop Med Hyg. 1974;23:8–14.
- Torrey EF, Torrey BB, Burton-Bradley BG. The epidemiology of schizophrenia in Papua New Guinea. Am J Psychiatry. 1974;131:567–572.
- Champfleury M. The Cat: Past and Present. (London: George Bell & Sons) 1885.
- Torrey EF and Miller J. The Invisible Plague: The Rise of Mental Illness from 1750 to the Present. (New Brunswick, N.J.: Rutgers University Press) 2001.
- Mortensen PB, Pedersen CB, Westergaard T, et al. Effects of family history and place and season of birth on the risk of schizophrenia. N Engl J Med. 1999;340:603–608.
- Hall S, Ryan M, Buxton D. The epidemiology of Toxoplasma infection. In Joynson DHM, Wreghitt TG, eds. Toxoplasmosis: A Comprehensive Clinical Guide. Cambridge: Cambridge University Press; 2001:58–124.
- Uga S, et al. Prevalence of Toxocara species eggs in the sandpits of public parks in Hyogo Prefecture, Japan. Jpn J Parasitol. 1989; 38(5): 280-284.
- Guebre-Xabier M, Nurilign A, Gebre-Hiwot A, et al. Sero-epidemiological survey of Toxoplasma gondii infection in Ethiopia. Ethiop Med. 1993;31:201–208.
- Bahia-Oliveira LMG, Jones JL, Azevedo-Silva J, et al. Highly endemic, waterborne toxoplasmosis in North Rio de Janeiro State, Brazil. Emerg Infect Dis. 2003;9:55–62.
- Jones JL, Kruszon-Moran D, Sanders-Lewis K, et al. Toxoplasma gondii infection in the United States, 1999–2004, decline from the prior decade. Am J Trop Med Hyg. 2007; 77:405–410.
- Forsgren M, Gille E, Ljungström I, et al.Toxoplasma gondii in pregnant women in Stockholm in 1969, 1979, and 1987 [letter]. Lancet. 1991;337:1413–1414.
- Walker J, Nokes DJ, Jennings R. Longitudinal study of Toxoplasma seroprevalence in South Yorkshire. Epidemiol Infect. 1992;108:99–106.
- Jones JL, Kruszon-Moran D, Sanders-Lewis K, et al. Toxoplasma gondii infection in the United States, 1999–2004, decline from the prior decade. Am J Trop Med Hyg. 2007;77:405–410.
- Wujcicka W, Gaj Z, Eilczynski J, Nowakowska D. Possible role of TLR4 and TLR9 SNPs in protection against congenital toxoplasmosis. Eur J Clin Microbiol Infect Dis. 2015; 34: 2121-2129.
- Shimokawa PT, Targa LS, Yamamoto L, et al. HLA-DQA1/B1 alleles as putative susceptibility markers in congenital toxoplasmosis. Virulence. 2016; 7: 456-464.
- Avramopoulous D, Pearce BD, McGrath J, et al. Infection and inflammation in schizophrenia and bipolar disorder: a genome wide study for interactions wit genetic variation. PLoS One. 2015; 10:e0116696.